She knew something was wrong the moment she noticed more hair than usual circling the drain after her shower.
At first, she brushed it off. Stress, maybe. A bad shampoo. But over the next several months, her ponytail felt thinner. Her part looked wider. And then came the chin hairs—coarse, dark, and suddenly requiring daily attention.
When she finally brought it up to her doctor, the response was confusing and frustrating:
“Your labs look fine. Your testosterone is normal. Your DHT is a little elevated, though—we could try finasteride.”
She left feeling dismissed. She didn’t want to jump straight to a medication that fully blocks a hormone pathway without understanding why this was happening in the first place. She wanted to know what was going on underneath—and whether there was a way to support her body rather than shut it down.
If this story feels familiar, you are not alone.
Why hair loss and androgen symptoms show up in perimenopause
During perimenopause and menopause, hormones don’t just “drop”—they change how they are processed in the body.
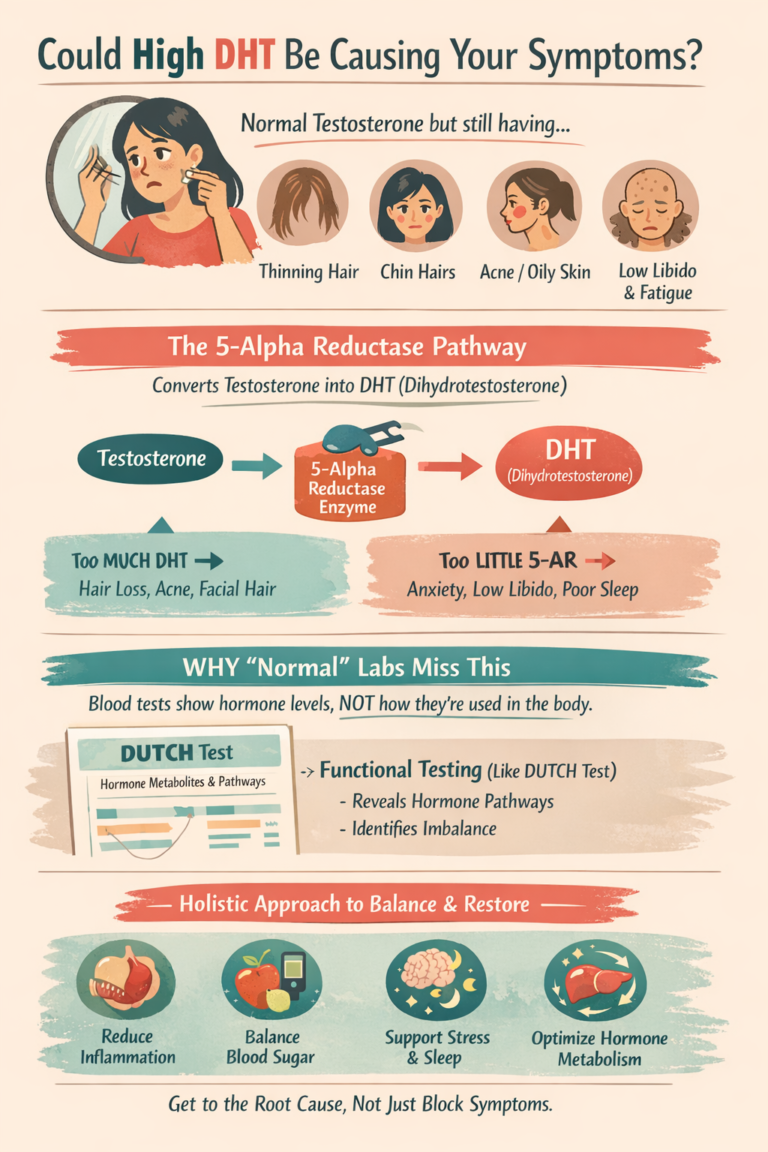
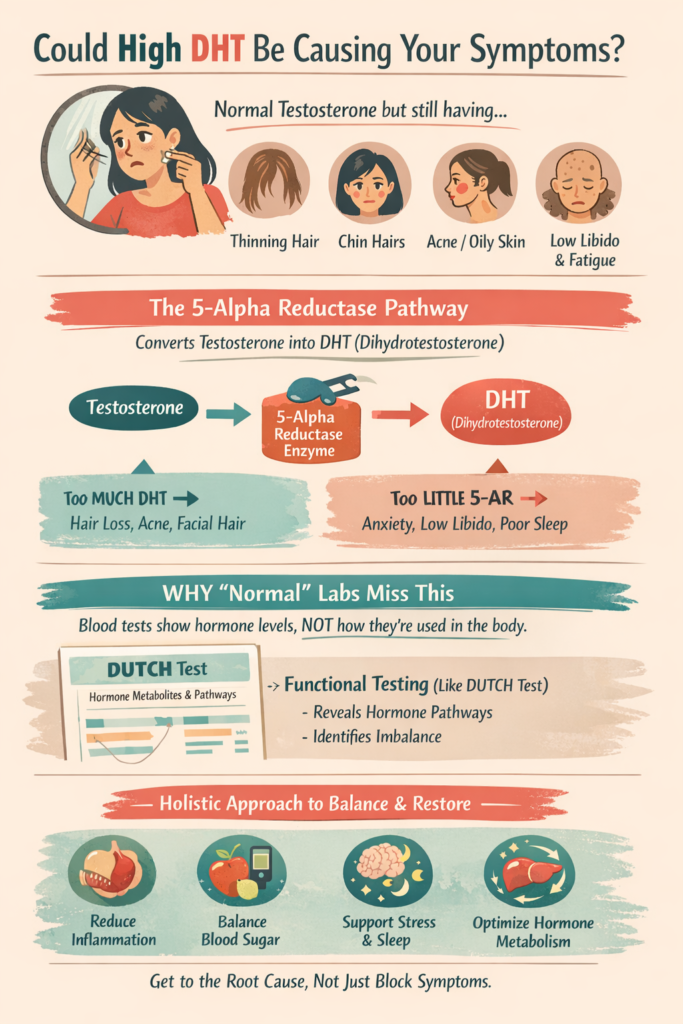
Even when testosterone levels are technically “within range,” women can still experience:
- Thinning hair on the scalp
- Increased facial or body hair
- Jawline acne or oily skin
- Irritability or mood changes
One of the most overlooked reasons for this is how testosterone is being converted, not how much of it you have.
What is DHT—and why does it matter?
DHT (dihydrotestosterone) is a more potent form of testosterone. It plays important roles in the body, but it is also the hormone most strongly linked to:
- Scalp hair follicle shrinkage
- Oily skin and acne
- Facial hair growth
DHT is made when testosterone is converted by an enzyme called 5-alpha reductase.
This enzyme is active in:
- Hair follicles
- Skin and oil glands
- The nervous system
- The liver and other tissues
In other words, where and how this enzyme is working matters just as much as hormone levels themselves.
Why “normal testosterone” doesn’t always mean you’re in the clear
Here’s where things get confusing for many women.
You can have:
- Normal or even low testosterone
- Normal blood work overall
- And still have high DHT activity in tissues
Why? Because blood tests measure what’s circulating—not what’s happening inside your tissues.
If your body is preferentially converting testosterone down the DHT pathway, you may experience DHT-type symptoms even when standard labs look “fine.”
This is especially common in perimenopause, when:
- Estrogen is declining or fluctuating
- Stress hormones are higher
- The body relies more on enzyme conversion than ovarian production
The role of 5-alpha reductase (and why it’s not the villain)
5-alpha reductase often gets labeled as “bad,” but it’s actually essential.
This enzyme is also involved in converting progesterone into calming brain chemicals (neurosteroids) that support:
- Sleep
- Mood stability
- Stress resilience
This is why fully blocking 5-alpha reductase with medications like finasteride can sometimes lead to:
- Anxiety or low mood
- Brain fog
- Low libido
- Worsened sleep
For many women, the problem isn’t that this pathway exists—it’s that it’s overactive or imbalanced.
Symptoms of 5-alpha reductase dysregulation
When activity is too high:
- Hair thinning or shedding on the scalp
- Chin or facial hair growth
- Acne or oily skin
- Irritability
When activity is too low:
- Low libido
- Anxiety or low mood
- Poor stress tolerance
- Sleep disturbances
Many perimenopausal women experience both at the same time, which is why symptoms can feel contradictory and confusing.
Why we can still be symptomatic even when labs are “normal”
Most routine blood tests do not show how hormones are being metabolized.
At Antigravity Wellness, we often see women with:
- Low or low-normal testosterone
- Low DHEA
- Yet clear signs of high DHT activity
This happens because the body is shunting hormones down certain pathways—something that standard blood work cannot fully capture.
A case story: “I finally felt like someone explained my body to me”
When we worked with this patient, we didn’t just rely on basic labs. We used a DUTCH hormone test, which looks at hormone metabolites and pathways over time.
Her results showed:
- Low androgen production overall
- A strong preference for the DHT (5-alpha) pathway
- Signs of stress-driven hormone conversion
Instead of blocking hormones, we focused on:
- Reducing inflammation
- Supporting blood sugar and stress regulation
- Improving nutrient status
- Calming the nervous system
- Supporting hormone metabolism and clearance
A few months later, she told us:
“My hair shedding slowed way down. My skin cleared. I finally started sleeping again. And for the first time in years, I felt like my body wasn’t fighting me.”
Only after her system was more balanced did we discuss whether gentle hormone support made sense for her.
How we approach this at Antigravity Wellness
We don’t believe in one-size-fits-all hormone care.
Our approach looks at:
- Symptoms and labs
- Blood work and, when appropriate, functional testing
- Hormone levels and how your body uses them
For women with hair loss, acne, or androgen-related symptoms in perimenopause or menopause, we focus on:
- Understanding hormone pathways
- Supporting the body before suppressing it
- Preserving brain, mood, and sexual health
Are you wondering if this applies to you?
If you are a woman living in Washington or Oregon and are struggling with symptoms like hair loss, chin hairs, acne, or feeling dismissed despite “normal labs,” we may be able to help.
👉 Take our Readiness Questionnaire to learn what next steps might look like and whether our clinic is a good fit for you.
Medical disclaimer
This article is for educational purposes only and is not intended as medical advice. It does not replace individualized care from a qualified healthcare provider. Always consult with your personal provider before starting or changing any treatment.
Medical references
- Handelsman DJ. Androgen physiology, pharmacology, use and misuse. Endocrine Reviews. https://www.ncbi.nlm.nih.gov/books/NBK279000/
- Labrie F et al. Intracrinology: Role of DHT in women. Hormone Molecular Biology and Clinical Investigation. https://academic.oup.com/edrv/article/24/2/152/2424204
- Peter J. Snyder et al. The Role of Androgens in Women. https://academic.oup.com/jcem/article-abstract/86/3/1006/2847441
- Silvia Diviccaro. Allopregnanolone: An overview on its synthesis and effects. https://pmc.ncbi.nlm.nih.gov/articles/PMC9285581/
- Richard S. Legro. Androgen excess disorders in women. New England Journal of Medicine. https://link.springer.com/chapter/10.1007/978-1-59259-388-0_7